
WHAT IS LAMINITIS
Laminitis results from inflammation of the sensitive laminae of the hoof.
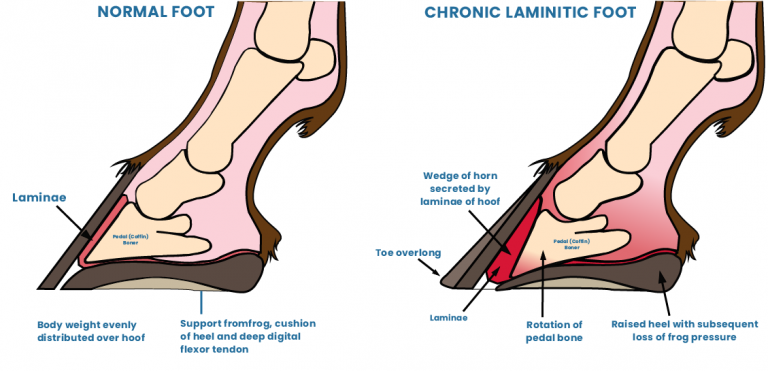
The laminae of the hoof are tiny interlocking finger-like projections that hold tightly together like a zipper. Their function within the foot is to securely attach the coffin (or pedal) bone to the hoof wall. Inflammation can permanently weaken these laminae and result in detachment of the strong bond between the hoof wall and the bone. The condition is very painful for the horse and in severe cases as the bone and the hoof wall separate, the coffin bone can rotate within the foot, may be displaced downward and eventually penetrate the sole. Laminitis may affect one or all feet, but it is most often seen in both front feet.
WHAT CAUSES LAMINITIS?
The causes of laminitis can be categorised into three groups; (1) Endocrine (hormone) associated (2) Systemic inflammatory response syndrome (SIRS) associated with inflammation or sepsis, and (3) mechanical overload.
(1) ENDOCRINE ASSOCIATED
This type accounts for around 90% of all cases of laminitis. This has to do with hormone regulation within the body.
There are two hormone associated conditions that contribute to laminitis: Equine Metabolic Syndrome (EMS) and Pars Pituitary Intermedia Dysfunction (PPID or Cushing’s disease).
Both these conditions are associated with the inbalance of insulin, which is also thought to be the underlying factor in endocrine associated laminitis. These horses will either have an elevated baseline level of insulin or an exaggerated insulin response to lush green grass or high grain feeds in the diet.
So far, we understand that insulin affects both the blood flow to laminae of the hoof and how the cells of the lamellae function. Hormone associated cases of laminitis will generally have multiple episodes of laminitis over many years. These often begin as very mild episodes but tend to become more frequent and severe over time. Steroid medications have also been linked to laminitis so care should be taken when steroids are administered at high levels, over long periods of time or to at risk horses.
(2) SIRS (SYSTEMATIC INFLAMMATORY RESPONSE SYNDROME) ASSOCIATED
We used to refer to this as ‘sepsis associated laminitis’, which is an inflammatory response to toxins being released into the blood stream. This is because it usually occurred as a response to bacterial infections such as pleuropneumonia (infection of the lungs), colitis (diarrhoea or inflammation of the gut) or endometritis (infection or inflammation in the lining of the uterus).
However, SIRS can also occur WITHOUT infection or sepsis, for example exposure to carbohydrate overload if a horse breaks into the feed shed and eats too much grain. The inflammation response in the body can affect multiple organs but also causes inflammation and breakdown of the tight bonds between the lamellae of the hoof capsule and coffin bone. Many of the SIRS associated cases have a very rapid onset. The horse will develop an increase in the digital pulses to the foot, will frequently weight shift and the condition will rapidly become very painful.
(3) MECHANICAL LAMINITIS
Laminitis can also develop due to excessive force on the hoof such as seen with “road founder” where the horse is ridden or driven on hard surfaces, causing inflammation and damage to the lamellae.
Another example is called supporting limb laminitis. This occurs when the horse is very lame on one leg and is reluctant to bear weight on the painful limb and places all its weight on the opposite leg. This supporting limb can develop laminitis due to excessive weight bearing, causing reduced blood supply the foot which compromises the lamellae. These horses need to be monitored closely as supporting limb laminitis can be missed initially as the horse is so lame on the opposite limb that it is not until the injured leg starts to improve or the laminitis has become very severe that it is diagnosed.
DIAGNOSIS
Signs of laminitis include the following:
- Lameness, especially when a horse is turning in circles.
- Constant weight shifting when standing.
- Heat in the feet.
- Increased digital pulse in the feet (this can be easily palpated over the sesamoid bones at the level of the fetlock).
- Pain in the toe region when pressure is applied with hoof testers.
- Reluctant or hesitant gait.
- A “sawhorse stance,” with the front feet stretched out in front to alleviate pressure on the toes and the hind feet positioned under them to support the weight that their front feet cannot.
Signs of chronic laminitis may include the following:
- Rings on the hoof wall that become wider as they are followed from toe to heel.
- Bruised soles.
- Widened/stretched white line.
- Frequent occurrence of hoof abscesses particularly over the toe region.
- Dropped soles with a convex appearance or ‘flat feet’.


TREATMENT
The sooner treatment begins, the better the chance for recovery. Treatment will depend on specific circumstances but may include the following:
- Diagnosing and treating the primary problem (e.g. an infection, Cushing’s disease etc).
- Icing the feet in acute cases.
- Dietary restrictions; stop feeding all grain-based feeds and stop access to lush pasture, feeding only soaked hay etc.
- Administering anti-inflammatory drugs like Bute to treat the pain and inflammation.
- Stabling the horse on soft ground, such as in sand or deep shavings, to provide support for the hoof. This can also encourage the horse to lie down reducing weight and pressure on the weakened laminae within the hoof capsule.
- Opening and draining any abscesses/seromas that may develop in the hoof.
- Cooperation between your veterinarian and the farrier (this can include corrective trimming, frog and sole supports and therapeutic shoes).
PROGNOSIS
Some horses that develop laminitis make uneventful recoveries and go back to their previous level of ridden work. Unfortunately, others can suffer such severe and irreparable damage to their hooves that for humane reasons they must be euthanized.
Your vet can provide you with information about the severity of your horse’s laminitis based on x-rays, and the animal’s response to treatment. X-rays will show how much rotation of the coffin bone has occurred, the severity of any separation of the lamellae and may also show up any other issues like painful hoof abscesses/seromas or changes to the coffin bone. All this information will help your vet formulate the best treatment plan for your horse and is essential to help your farrier set your horse up with the correct therapeutic shoeing. Repeat x-rays may be taken over time to assess the response to treatment and help plan your horses on-going management.
MANAGEMENT
It is important to note that once a horse has had laminitis, it may be more likely to reoccur. Many cases persist for a long time or even a life time, because the pedal bone or laminae have become permanently damaged or due to ongoing conditions requiring management such as PPID. Extra care is recommended for any horse that has had laminitis before, including:
- A modified diet that provides adequate nutrition but avoids excess carbohydrates.
- Routine hoof care, including regular trimming and, in some cases, therapeutic shoeing (x-rays may be needed to monitor progress over time).
- A good general health-maintenance schedule.
- Possibly a nutritional supplement formulated to promote hoof health.
- Restrict pasture intake during spring or anytime the pasture becomes lush and green.
The best way to deal with laminitis is by preventing the causes under your control. Keep all grain stored securely out of the reach of horses. Introduce your horse to lush pasture gradually. Be aware that when a horse is ill, under stress or overweight, it is especially at risk. Formulate a good dietary plan. Provide routine health and hoof care. If you suspect laminitis, consider it a medical emergency, and notify your veterinarian immediately.




